Idiopathic inflammatory myopathy of older adults characterized by progressive muscle weakness and rimmed vacuoles (inclusion bodies) on muscle biopsy.
Most common acquired muscle disease in patients >50. Often misdiagnosed as polymyositis, it causes significant disability (many patients become wheelchair-dependent with severe dysphagia) and does not respond to standard immunosuppressive therapy—making early recognition and supportive management crucial.
Age >50, usually male, with insidious (years-long) muscle weakness. IBM uniquely involves both proximal muscles (e.g. quadriceps → difficulty rising, frequent falls) and distal muscles (e.g. finger flexors → weak grip), often asymmetric in distribution. Patients may have knee buckling falls or foot drop causing tripping, along with trouble using their hands for fine tasks.
Slow progression (often ~5 years before diagnosis) with visible muscle atrophy in affected groups (thigh, forearm) even early on. About 30–50% develop dysphagia (difficulty swallowing) due to pharyngeal muscle involvement, leading to choking or aspiration pneumonia risk.
Labs: Serum CK is normal or only mildly elevated (typically <10× normal). No myositis-specific antibodies (e.g. Jo-1) are present, but ~50% of patients have anti-NT5c1A (anti-cytosolic 5′-nucleotidase 1A) antibodies. Inflammatory markers (ESR, CRP) are often normal.
Suspect IBM (instead of polymyositis) if an older patient's myopathy has atypical features (distal weakness, asymmetry, very slow course) or fails to improve with therapy.
Use EMG to confirm a myopathic process and exclude neuropathic causes. MRI of muscles can show characteristic patterns (selective quadriceps and forearm flexor involvement) and help target a biopsy site.
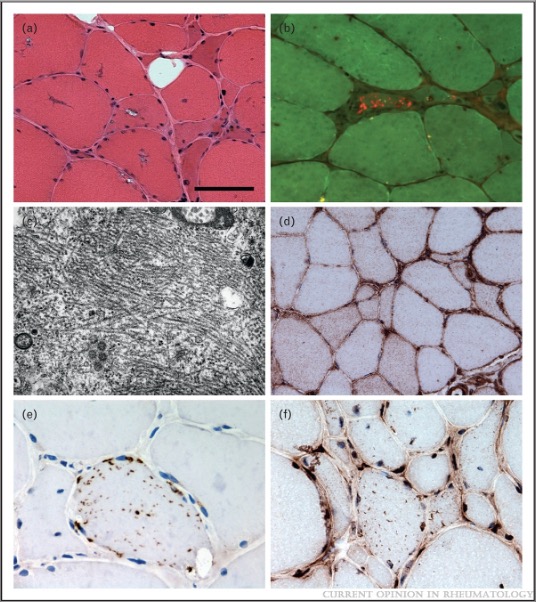
Muscle biopsy is the diagnostic gold standard: look for endomysial CD8+ T-cell infiltrates with muscle fiber degeneration, rimmed vacuoles, and protein aggregates (inclusion bodies). These findings confirm IBM and distinguish it from polymyositis (which lacks inclusions).
If IBM is confirmed, avoid prolonged courses of corticosteroids or other immunosuppressants (ineffective) and focus on supportive care.
Proximal weakness with characteristic skin rash (heliotrope, Gottron papules); path shows perifascicular atrophy; higher risk of malignancy (unlike IBM).
Muscular dystrophies
Hereditary muscle diseases (e.g. Duchenne, myotonic dystrophy) with earlier onset and family history; typically no inflammatory cells on biopsy (and often different patterns like calf pseudohypertrophy or myotonia).
No proven cure - IBM is generally refractory to corticosteroids and immunosuppressants (unlike polymyositis). Management is primarily supportive and rehabilitative.
Exercise and physical therapy to preserve muscle function; provide assistive devices (e.g. ankle-foot orthoses for foot drop, canes/walkers, wheelchairs) to improve mobility and prevent falls.
Manage dysphagia with dietary modifications (soft or thickened foods) and swallowing therapy; if severe, consider feeding tube placement to prevent aspiration. Monitor respiratory status in advanced cases (aspiration precautions, pulmonary support if needed).
Think of IBM the company: it's old and doesn't adapt to change – similarly, Inclusion Body Myositis affects older patients and is resistant to standard treatments.
Mnemonic "IBM" – Inclusions in muscle fibers (rimmed vacuoles), Both proximal & distal muscle involvement, Male-predominant (midlife) and Medications don't work (steroid-unresponsive).
Progressive dysphagia (choking, coughing with meals) → risk of aspiration pneumonia; warrants prompt evaluation (swallow study) and interventions (diet changes, feeding tube).
Frequent falls or trips (due to quadriceps weakness or foot drop) → high injury risk; ensure use of assistive devices and home safety measures (to prevent fractures/head injury).
Chronic muscle weakness (>6–12 months) in age >50 → check CK (often mildly elevated) and basic myositis antibody panel; consider IBM if distal involvement or atypical features present.
Obtain EMG to support a myopathy (and rule out neurogenic causes) and perform muscle MRI to identify affected muscles (IBM shows selective quadriceps and finger flexor atrophy) and guide biopsy site selection.
Biopsy an affected muscle to confirm the diagnosis: presence of endomysial inflammation plus rimmed vacuoles and inclusions establishes IBM.
If diagnosis is IBM, focus on supportive management (rehabilitation, safety, swallowing support) rather than high-dose immunosuppression (ineffective in IBM).
Older adult (≥60) with slowly progressive thigh weakness (difficulty climbing stairs, frequent falls) and forearm/finger weakness (poor grip), modest CK elevation, and no improvement on steroids → Inclusion body myositis.
Muscle biopsy photomicrograph showing fibers with rimmed vacuoles (blue-red granular holes on trichrome stain) in an older patient with chronic muscle weakness → Inclusion body myositis.
Case 1
A 68-year-old man has a 2-year history of progressive difficulty climbing stairs and recently developed trouble opening jars and frequent falls.
Muscle biopsy in inclusion body myositis showing fibers with rimmed vacuoles (inclusion bodies).