X-linked recessivedystrophin gene mutation causing absent dystrophin protein and progressive muscle fiber degeneration.
Most common fatal childhood muscular dystrophy; boys develop early weakness and lose ambulation by adolescence. Complications (cardiomyopathy, respiratory failure) lead to death in early adulthood.
Toddler/young boy with delayed motor milestones (late walking) and proximal muscle weakness (trouble climbing, frequent falls).
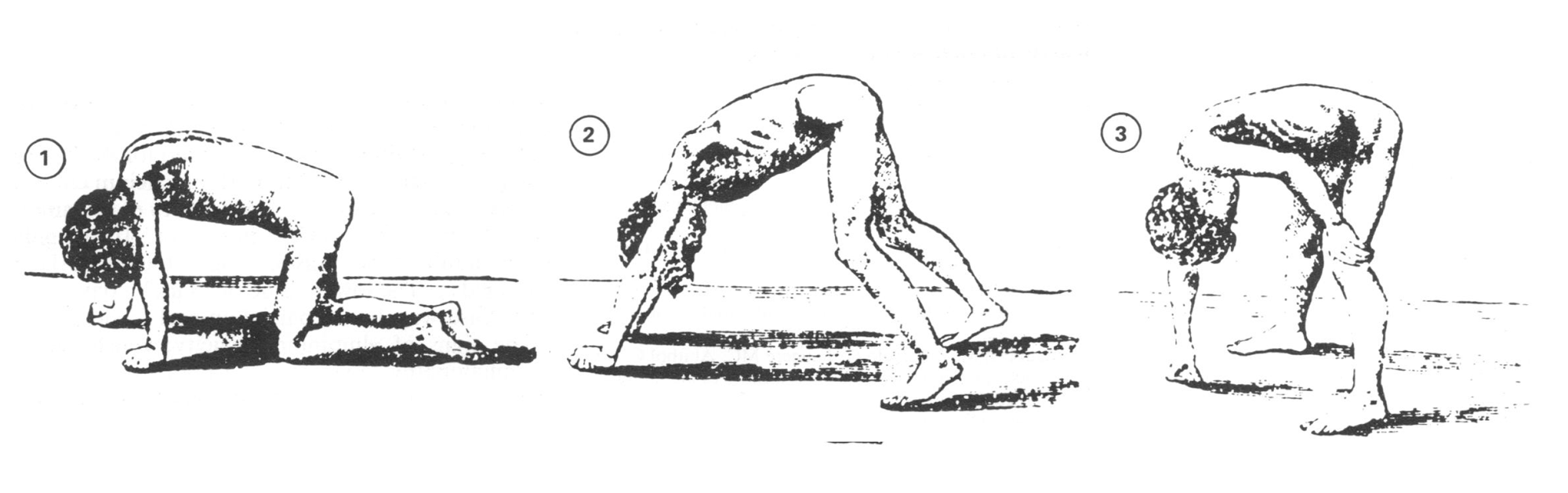
Waddling gait, lumbar lordosis, and Gowers sign (using hands to "climb" up legs when standing) by age 3–6.
Calf pseudohypertrophy (enlarged calves from fat/connective tissue) appears a bit later. Eventual wheelchair dependence by ~age 12.
If you suspect DMD, check CK level – it will be massively elevated (often >10× normal).
Confirm diagnosis with genetic testing for DMD gene deletions/variants (e.g., multiplex PCR or MLPA). Muscle biopsy (immunostaining or Western blot) shows absent dystrophin if genetic testing is inconclusive.
Assess cardiac and respiratory status at baseline (echocardiogram, pulmonary function tests), and offer genetic counseling (mother & female relatives may be carriers).
Condition
Distinguishing Feature
Becker muscular dystrophy
later onset (teens or adulthood), partial dystrophin (in-frame mutations) → milder course
Spinal muscular atrophy
infantile or childhood onset, proximal weakness from anterior horncell degeneration (LMN signs, fasciculations); normal dystrophin gene
Cerebral palsy
non-progressive, early motor delay due to brain injury (often spasticity & hyperreflexia, normal CK)
Glucocorticoids (e.g., prednisone or deflazacort) are the mainstay – they slow muscle degeneration and prolong ambulation.
Exon skipping therapies (e.g., antisense oligonucleotides like eteplirsen) can allow production of partial dystrophin for certain mutations.
Supportive care: Physical therapy and bracing to improve mobility and prevent contractures; pulmonary support (e.g., nighttime ventilation) as respiratory muscles weaken; cardiac management (ACE inhibitors, beta-blockers) to delay heart failure.
New prospects: experimental gene therapies (micro-dystrophin viral vectors) are under investigation.
Mnemonic: Duchenne = Deleted Dystrophin (frameshift or nonsense mutation → no protein); Becker = Bad but not absent (some protein, hence milder).
Gowers sign tip: child uses arms to climb up their body due to weak legs.
DMD gene is the largest human gene (~2.2 Mb) → high mutation rate (≈1/3 cases from new mutations).
Avoid succinylcholine in DMD patients (risk of life-threatening rhabdo or malignant hyperthermia-like reaction under anesthesia).
Signs of nighttime hypoventilation (morning headaches, daytime sleepiness) in a DMD patient → initiate noninvasive ventilation (BiPAP) to prevent respiratory failure.
Acute heart failure or arrhythmia in a DMD patient → evaluate and treat for dilated cardiomyopathy (a common late complication).
Young boy with motor delay or proximal weakness → check serum CK (markedly elevated in DMD).
If CK is high → perform genetic test for DMD gene mutation to confirm Duchenne MD.
Consider muscle biopsy if genetic testing is negative or unavailable (dystrophin immunostaining).
After diagnosis: start steroids if appropriate, monitor heart (echos) & lungs (PFTs) regularly, and provide family genetic counseling.
A 4‑year‑old boy with delayed walking, frequent falls, and using his hands to push on his legs to stand (positive Gowers sign); exam shows calf enlargement → Duchenne muscular dystrophy.
Teen male with history of Duchenne MD now presents with chest pain and dyspnea; EKG shows arrhythmia, echo shows dilated cardiomyopathy → DMD-associated cardiomyopathy (common in late-stage DMD).
Case 1
A 4‑year‑old boy is brought in for frequent falls and difficulty standing up from the floor.
Case 2
A 17‑year‑old with Duchenne muscular dystrophy presents with worsening shortness of breath and leg swelling.
Sequence of a child using hands on legs to stand (positive Gowers sign in Duchenne MD).