Contagious rubella virus infection ("German measles") causing a mild 3-day rash and fever. Congenital rubella syndrome (CRS) refers to the constellation of birth defects (e.g., deafness, cataracts, heart defects) from in utero infection.
Rubella is the leading vaccine-preventable cause of birth defects worldwide. Infection in pregnancy often leads to miscarriage or severe fetal anomalies (CRS), making rubella immunity and vaccination critically important.
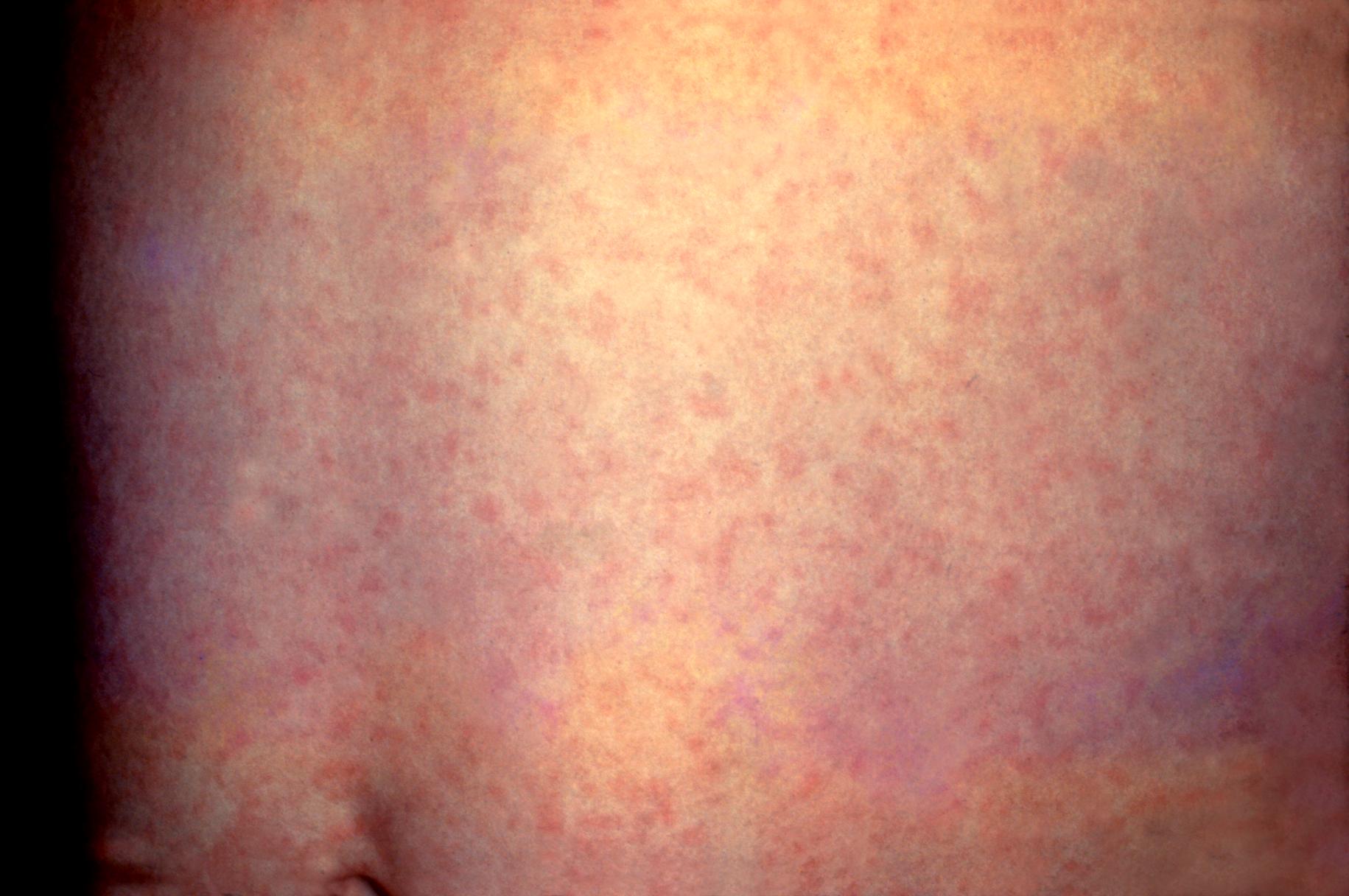
Child with pink maculopapular rash starting on face → spreads down the body, fading by ~3 days; low fever or none; tender posterior auricular & suboccipital lymphadenopathy is characteristic.
Adults (especially women) often get polyarthritis (up to 70%) along with the rash. Many infections (25–50%) are asymptomatic.
Congenital rubella: newborn with classic triad of cataracts, sensorineural deafness, and PDA (heart defect), often with a "blueberry muffin" rash (purpuric spots from extramedullary hematopoiesis).
Confirm diagnosis with labs: rubella-specific IgM antibody or a ≥4-fold rise in IgG titer between acute & convalescent samples. RT-PCR can detect the virus in throat swabs, blood, or amniotic fluid.
In pregnant women, check rubella IgG status early (prenatal screening). If non-immune, avoid exposure and plan to give MMR vaccine after delivery (live rubella vaccine is contraindicated during pregnancy).
Suspected rubella cases should be isolated (droplet precautions) and reported to public health authorities. Patients are contagious ~1 week before to 1 week after rash onset, so keep affected kids out of school for 7 days post-rash.
For a neonate with possible CRS: test IgM (which indicates neonatal infection, since IgM doesn't cross placenta) and consider PCR. Persistence of rubella-specific IgG beyond 6–12 months (after maternal IgG wanes) also confirms congenital infection.
High fever, cough/coryza/conjunctivitis, Koplik spots; rash is darker, lasts >3 days
Parvovirus B19 (erythema infectiosum)
"Slapped-cheek" rash in kids; arthralgias in adults; can cause fetal hydrops in pregnancy
Roseola infantum (HHV-6)
Infants with high fever for 3–5 days then rash appears (trunk → extremities)
Scarlet fever
Group A Strep with sandpaper rash, strawberry tongue, and pharyngitis
No specific antiviral – supportive care only (rest, hydration, NSAIDs for fever or arthritis). Rubella is usually self-limited.
Avoid exposing pregnant contacts: patients with rubella should stay home (no school or work) for 7 days after rash onset to prevent spread.
Infants with CRS require supportive management of defects (e.g., surgery for cardiac defects or cataracts, hearing rehabilitation). They should be isolated, as they shed virus for ≥1 year.
Think Forchheimer spots: petechial red spots on the soft palate seen in ~20% of rubella cases.
Rubella vs. Rubeola: Rubella (German measles) is a different virus than measles and much milder (3-day rash, lower fever, lymph nodes) compared to measles' severe 7-day illness.
Rubella in early pregnancy (first trimester) → up to 90% chance of CRS in the fetus. This is a medical emergency in terms of counseling (high risk of miscarriage or severe birth defects).
Newborns with CRS shed rubella virus in urine/secretions for months – pose infection risk. Use contact precautions and keep them away from pregnant caregivers.
Fever & rash (face → body) with lymph nodes → suspect rubella (especially if unvaccinated).
Lab tests: draw rubella IgM (acute) and IgG (acute + 2-3 weeks later) to confirm; consider throat PCR.
Isolate the patient if rubella is likely (no school/work) and notify public health department.
If pregnant exposure: check maternal IgG/IgM ASAP. If infection confirmed in first trimester, counsel about high CRS risk (no treatment to prevent fetal damage).
Ensure MMR vaccination for prevention: 2 doses in childhood; non-immune adults (especially women) should receive it (postpone until after pregnancy if currently pregnant).
Unvaccinated child with a rash that started on the face and tender postauricular lymph nodes → rubella (German measles).
Pregnant woman with no MMR immunizations develops mild fever, rash, and lymphadenopathy in the first trimester → baby at risk for congenital rubella syndrome (deafness, cataracts, PDA).
Case 1
A 4-year-old boy who never received vaccines develops a rash that started on his face and spread downward over 3 days.
Case 2
An infant is born with cataracts, a heart murmur, and sensorineural hearing loss. His mother reports a flu-like illness with rash during the first trimester of pregnancy.
Rubella rash on a child's abdomen (pink maculopapular lesions of German measles).