Abnormally high white blood cell count (typically >11,000/µL in adults).
Alerts clinicians to underlying conditions (infection, inflammation, stress, or leukemia). Also, extremely high WBC counts can cause hyperviscosity (leukostasis) and often signify serious pathology.
Infection/inflammation: e.g. pneumonia or appendicitis with fever and WBC 15–25k (neutrophil predominance, left shift). Severe infections (sepsis, *C. diff* colitis) can cause WBC >50k (leukemoid reaction).
Hematologic malignancy: chronic leukemias (CML, CLL) often have very high WBC (e.g. >50–100k); patients may have splenomegaly, B symptoms (weight loss, night sweats) or be asymptomatic (incidental finding).
Medications/stress: corticosteroids (e.g. prednisone) cause neutrophil demargination leading to leukocytosis (typically 12–18k) without infection; intense stress (trauma, exercise) or epinephrine can transiently elevate WBC.
Interpret WBC with differential: identify which cell type is elevated (neutrophilia suggests bacterial infection or CML; lymphocytosis suggests viral infection or CLL; eosinophilia points to allergy/parasites, etc.).
Review the peripheral smear: the presence of blasts or very immature cells strongly suggests leukemia (not reactive); toxic granulation or Döhle bodies in neutrophils support infection.
If neutrophil count is markedly high with no obvious cause, check leukocyte alkaline phosphatase (LAP) score: high in reactive leukemoid reactions, but low in CML. CML often also has increased basophils.
For suspected leukemia, pursue definitive tests: e.g. send molecular test for BCR-ABL (Philadelphia chromosome) in suspected CML, and perform bone marrow biopsy with flow cytometry to confirm malignancy.
Condition
Distinguishing Feature
Leukemoid reaction
reactive neutrophilic leukocytosis (often >50k) from severe infection/inflammation; high LAP, no clonal markers
myeloproliferative neoplasm with extreme WBC (often >100k) + basophilia; BCR-ABL positive (Philadelphia chr); low LAP
Infection or inflammation
common cause of mild–moderate leukocytosis (e.g. bacterial pneumonia, appendicitis); usually WBC <30k and normalizes after illness
Corticosteroid effect
drug-induced neutrophilia (demargination); moderate WBC elevation without infection
Benign/reactive leukocytosis requires treating the underlying cause: e.g. antibiotics for infection, management of inflammation; the WBC count will normalize with resolution.
If drug-induced (e.g. steroid therapy), reduce or discontinue the offending medication if clinically appropriate.
Malignant leukocytosis (leukemia) warrants specific therapy for that leukemia (e.g. tyrosine kinase inhibitor such as imatinib for CML, or chemotherapy for acute leukemia).
If WBC is >100k with signs of leukostasis (dyspnea, neurologic deficits), initiate urgent measures to rapidly lower the count (e.g. IV hydroxyurea, leukapheresis).
LAP score mnemonic: Leukemoid = LAP high, Leukemia (CML) = LAP low.
Steroids cause neutrophils to demarginate (detach from blood vessel walls), raising the circulating WBC count without new cell production.
Blasts on peripheral smear (any significant blast presence) → highly suggestive of acute leukemia (requires immediate evaluation).
Extremely elevated WBC (e.g. >100,000/µL) with dyspnea, headache, or confusion → think hyperviscosity syndrome (leukostasis) — a medical emergency.
Leukocytosis accompanied by anemia, thrombocytopenia, or organomegaly (splenomegaly, lymphadenopathy) → concerning for leukemia or bone marrow disorder rather than a benign reaction.
↑WBC on lab → repeat CBC + differential to confirm and identify which lineage is elevated.
Clinical assessment → look for infection (fever, source), inflammation, stress or medications that could explain a reactive leukocytosis.
If neutrophilia with no clear cause → obtain a LAP score (high = reactive, low = CML) and consider molecular testing for BCR-ABL; treat any hidden infection if suspected.
If lymphocytosis → test for acute infection (e.g. EBV serologies); if persistent or extreme, get flow cytometry on blood to evaluate for clonal lymphoproliferative disorder (e.g. CLL).
No obvious benign cause or abnormal cells present → refer to hematology for bone marrow biopsy and cytogenetic studies to rule out leukemia.
Patient with severe *C. difficile* colitis, WBC 55,000 (neutrophils with bands), high LAP score → Leukemoid reaction due to infection.
Middle-aged adult with 100,000 WBC, left-shifted neutrophils + basophils, massive splenomegaly, low LAP → Chronic myelogenous leukemia (CML).
Asthma patient on high-dose prednisone with WBC 16,000 (mostly neutrophils, no fever or infection) → Steroid-induced leukocytosis.
Case 1
A 55‑year‑old hospitalized man with severe diarrhea from Clostridioides difficile infection is noted to have a WBC count of 52,000/µL.
Case 2
A 60‑year‑old man with fatigue and early satiety is found to have a WBC count of 110,000/µL on routine blood work.
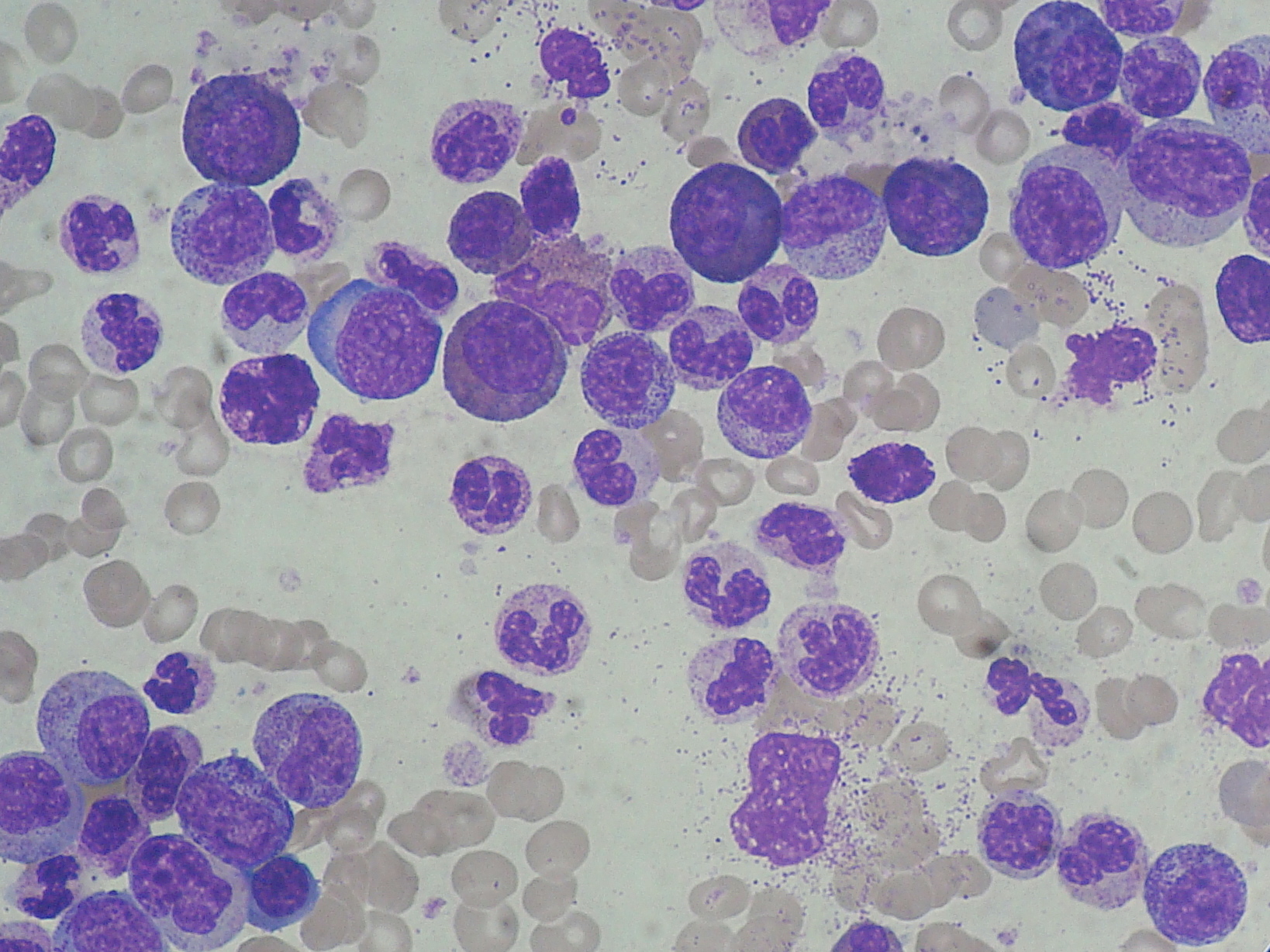
Chronic myeloid leukemia (CML) peripheral smear showing marked leukocytosis with granulocyte left shift.