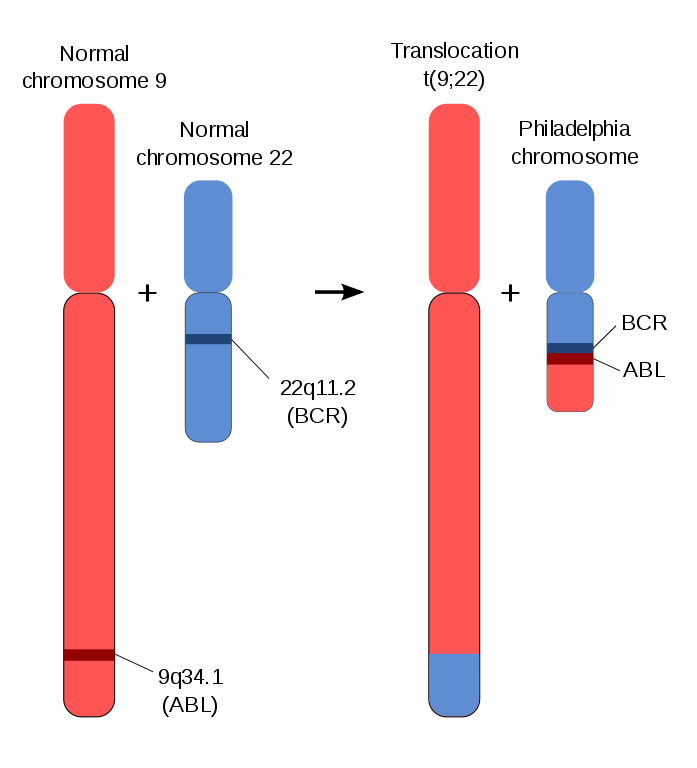
Myeloproliferative neoplasm with unchecked myeloid (granulocyte) proliferation; driven by BCR-ABL fusion (Philadelphia chromosome t(9;22)) leading to a constitutively active tyrosine kinase.
Revolutionized by targeted therapy (imatinib); untreated CML can progress to a fatal blast crisis (acute leukemia). Often cited as a classic example linking a specific mutation (Ph chromosome) to cancer and demonstrating dramatic treatment success.
Often asymptomatic until noted incidentally on labs (WBC >100,000) in a middle-aged adult.
If symptomatic: fatigue, weight loss, night sweats, and splenomegaly (early satiety, LUQ fullness) are common.
Labs: marked leukocytosis with left-shifted neutrophils (from myeloblasts to segs) and often basophilia; platelets can also be elevated.
Differentiate CML from leukemoid reaction (infection) with leukocyte alkaline phosphatase (LAP) score: CML neutrophils have low LAP (vs high in reactive leukemoid).
Confirm diagnosis with genetic testing: look for Philadelphia chromosome on karyotype or BCR-ABL1 fusion via PCR.
Classify phase by blast %: chronic (<10% blasts), accelerated (~10–19%), or blast crisis (≥20% blasts, acute leukemia transformation).
acute leukemia with >20% blasts, abrupt onset, more severe cytopenias
Tyrosine kinase inhibitors (e.g., imatinib) are first-line, targeting the BCR-ABL oncoprotein to induce remission.
If resistance (e.g., T315I mutation) or progression: switch to a different TKI (dasatinib, nilotinib; ponatinib for T315I) or proceed to allogeneic stem cell transplant.
Blast phase is treated like acute leukemia (TKI + conventional chemo), often followed by transplant.
Mnemonic: Philadelphia CreaML cheese (Philadelphia chromosome = CML).
LAP is Low in Leukemia (CML) but high in leukemoid reactions.
Rising blast count (≥20%) or new cytopenias in a CML patient → progression to advanced phase (accelerated or blast crisis).
Sudden worsening symptoms (fevers, bone pain, rapidly enlarging spleen) despite therapy → evaluate for blast transformation.
Order confirmatory testing: cytogenetics for Ph chromosome or PCR for BCR-ABL1.
If positive, assess disease phase (chronic vs accelerated vs blast) by blast percentage and clinical features.
Start imatinib (or another TKI) for chronic phase and monitor BCR-ABL levels for response.
If inadequate response or progression → change to second-line TKI or refer for transplant evaluation.
Middle-aged patient with massive splenomegaly, WBC ~100,000 (mostly neutrophils with left shift, plus basophils) and low LAP → CML (chronic phase, Ph chromosome).
CML patient on imatinib with fatigue, fever, bone pain, and 25% blasts on blood smear → blast crisis (acute transformation requiring aggressive therapy).
Case 1
A 52‑year‑old man is evaluated for fatigue and early satiety.
Case 2
A 45‑year‑old woman with known CML on therapy develops fever and bone pain.
Diagram of the Philadelphia chromosome translocation (BCR-ABL fusion on chromosomes 9 and 22).