Atherosclerotic occlusion at the aortic bifurcation (distal aorta or common iliac arteries) causing the classic triad of buttock claudication, diminished femoral pulses, and erectile dysfunction.
Represents severe peripheral artery disease at the aortoiliac level, leading to significant morbidity (walking impairment, sexual dysfunction) and indicating widespread atherosclerosis. Recognizing this syndrome can prompt timely revascularization to prevent progression to critical limb ischemia.
Classically occurs in older male smokers with bilateral hip, thigh, and buttock claudication that is relieved by rest.
On exam, femoral pulses are weak or absent, often with signs of chronic poor perfusion (cool, hairless lower extremities). Erectile dysfunction in men is a key clue (due to impaired internal iliac flow).
Risk factors are those of atherosclerosis: smoking, hypertension, hyperlipidemia, diabetes, etc. Some patients remain asymptomatic due to collateral circulation until disease is advanced.
Differentiate vascular claudication from neurogenic claudication: Leriche's leg pain comes from ischemic muscle, consistently triggered by exercise and relieved with standing rest; spinal canal stenosis causes neurogenic claudication relieved by flexion ("shopping cart" sign) and usually normal pulses.
Measure ankle-brachial index (ABI): ABI <0.90 confirms PAD (often <0.50 in severe aortoiliac disease). If ABI is normal but suspicion remains high, exercise ABI testing can unmask occlusive disease.
Localize the lesion: a pulse drop between brachial and femoral pulses suggests aortoiliac disease. Arterial Doppler ultrasound can detect flow limitations; CTA or MRA can map the occlusion for intervention.
Assess for limb-threatening features: rest pain, ischemic ulcers, or gangrene signal critical limb ischemia and urgent need for revascularization.
Condition
Distinguishing Feature
Lumbar spinal stenosis
neurogenic claudication – leg pain with walking that improves when bending forward; normal leg pulses
Distal PAD (femoropopliteal disease)
atherosclerosis confined to femoral/popliteal arteries – calf claudication only, femoral pulses intact, no impotence
Risk factor optimization: smoking cessation, exercise training, and medical therapy (statin, antiplatelet, control of diabetes/HTN) to slow atherosclerosis and improve claudication.
Revascularization for lifestyle-limiting claudication or critical ischemia: options include endovascular angioplasty with stenting (e.g., bilateral "kissing" iliac stents) or surgical bypass (aortobifemoral bypass graft is gold-standard for long-term patency; axillo-femoral and fem-fem bypass are alternatives if aortic surgery is high-risk).
For claudication symptoms not severe enough for surgery, cilostazol (a PDE3 inhibitor) can improve walking distance (unless contraindicated by heart failure). Address erectile dysfunction with PDE5 inhibitors if needed, though improving pelvic flow via revascularization may help.
Remember Leriche's triad: buttock claudication, impotence, and absent femoral pulses (think C‑I‑A for claudication, impotence, absent pulses at the common iliac arteries).
Chronic aortoiliac occlusion rarely causes acute limb ischemia because collateral circulation develops over time. Sudden bilateral leg ischemia should raise concern for an acute aortic occlusion (embolus or thrombosis).
Rest pain, foot ulcers, or gangrene (critical limb ischemia) → requires urgent revascularization to prevent limb loss.
Acute aortic occlusion (e.g., saddle embolus or thrombosis at the bifurcation) causes sudden bilateral leg pain, paralysis, and loss of pulses – a surgical emergency.
Exertional leg pain in a patient with vascular risk factors → examine pulses and measure ABI to confirm peripheral arterial disease.
If aortoiliac occlusion suspected (low ABI, diminished femoral pulses, Leriche triad) → initiate risk factor control (quit smoking, statin, etc.) and evaluate severity.
Obtain arterial imaging (Duplex ultrasound initially; CTA/MRA for detailed mapping) if intervention is considered or if diagnosis is unclear.
Claudication management: trial of exercise therapy and medications. If severe functional limitation or any signs of critical ischemia → refer to vascular surgery for revascularization (endovascular vs. surgical).
Post-intervention: continue risk factor management and surveillance for graft or stent patency (regular pulse exams, ultrasounds as needed).
Middle-aged male smoker with buttock and thigh pain on exertion, erectile dysfunction, and absent femoral pulses → Aortoiliac occlusive disease (Leriche syndrome).
Case 1
A 55‑year‑old man with a 40-pack-year smoking history reports pain in his buttocks and thighs after walking two blocks, which forces him to stop and rest.
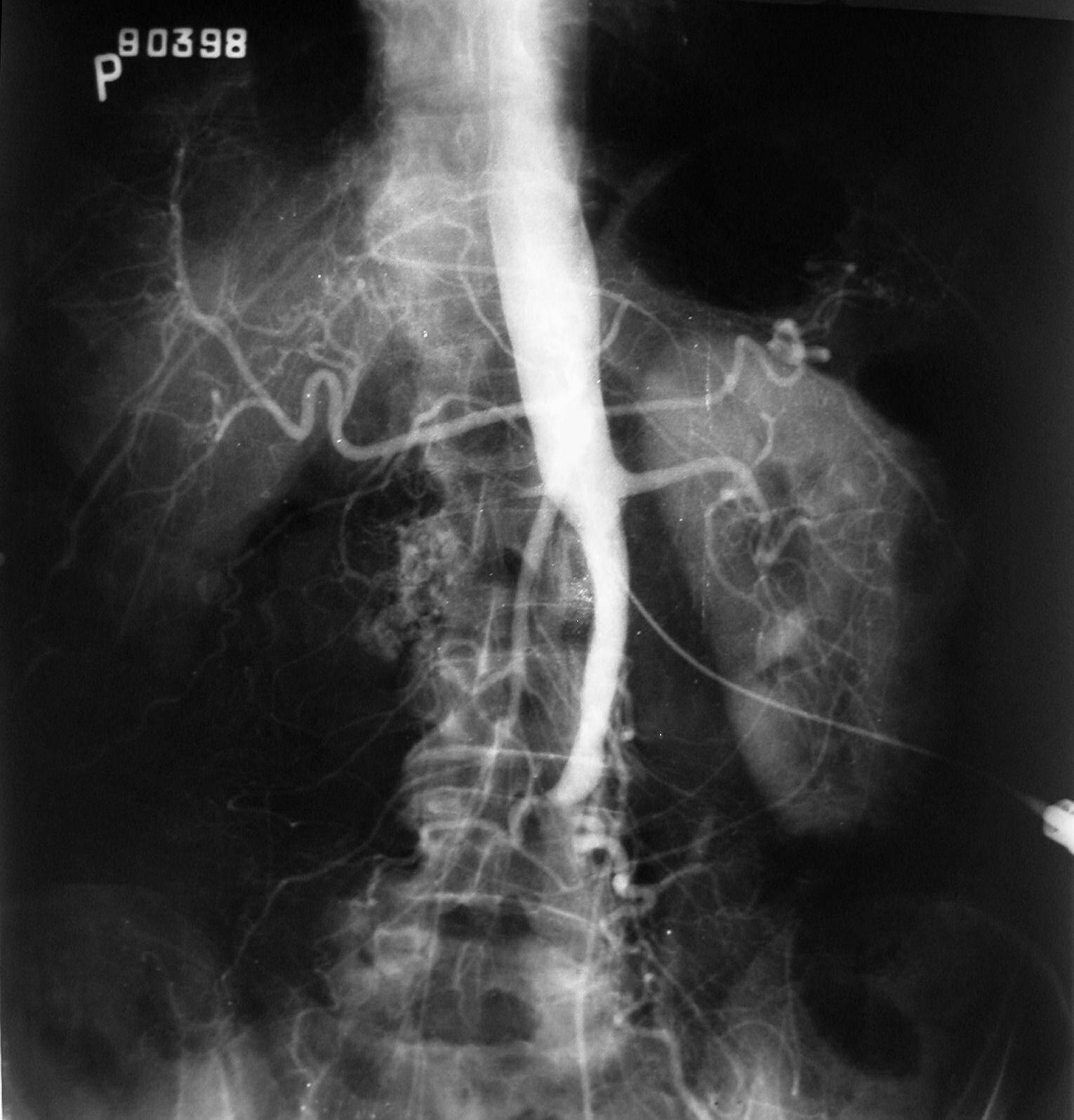
Fluoroscopic angiogram showing complete occlusion of the distal aorta at its bifurcation (Leriche syndrome). No contrast fills the iliac arteries.