Severe protein malnutrition in children characterized by bilateral pitting edema and fatty liver (distended abdomen).
Life-threatening if untreated (undernutrition underlies ~45% of under-5 child deaths) and a classic exam example of severe malnutrition (often contrasted with marasmus).
Typically in a child ~1–3 years old, post-weaning (e.g., older sibling displaced from breastfeeding when a new baby arrives) with a diet high in starch but extremely low in protein. Common in extreme poverty or famine, often precipitated by an infection (e.g., measles, chronic diarrhea) that worsens nutrition.
Hallmark edema: bilateral pitting edema in legs/feet (can progress to generalized anasarca) with a swollen abdomen (hepatomegaly from fatty liver). Children may appear plump or of normal weight due to fluid retention, masking severe muscle wasting.
Skin and hair changes: patchy hyperpigmented rash with desquamation (peeling, 'flaky paint' skin); hair becomes thin, brittle, and reddish or depigmented (may show a 'flag sign' banding).
Behavior: malnourished children are often irritable, apathetic, and have poor appetite (anorexia) (unlike marasmus, where appetite is usually preserved).
Assess nutritional status: measure MUAC and weight-for-height. MUAC < 11.5 cm or weight-for-height < –3 SD = severe acute malnutrition. Bilateral pitting edema (of nutritional origin) also defines SAM (kwashiorkor) even if weight is normal.
Rule out other edema causes: e.g., check urine for protein to exclude nephrotic syndrome. In kwashiorkor, edema occurs without another cause and in context of obvious malnutrition (hair/skin changes, etc.).
Decide inpatient vs outpatient: Any edema, poor appetite, or acute complication (infection, shock, etc.) = complicated SAM → admit for inpatient care. If child is alert, with good appetite and no edema or complications = uncomplicated SAM → manage with outpatient therapeutic feeding.
Differentiate kwashiorkor vs marasmus: both are severe PEM, but marasmus is severe wasting without edema (a frail, emaciated child). Management principles overlap (careful refeeding, infection treatment), though kwashiorkor tends to have more urgent complications (edema, hypoglycemia, etc.).
edema from kidney protein loss (massive proteinuria); no hair/skin changes of malnutrition
Stabilization first: treat hypoglycemia (immediate feeding or IV 10% dextrose) and hypothermia (keep warm) as they often coexist with infection. Start broad antibiotics empirically (assuming hidden infection).
Rehydrate carefully: malnourished children have reduced cardiac reserve. Use oral rehydration slowly (low-sodiumReSoMal solution); avoid IV fluids unless in shock (risk of fluid overload).
Provide micronutrients: give vitamin A on admission (especially if measles or eye signs of deficiency) and daily multivitamins. Correct electrolyte deficiencies (low potassium, magnesium, etc.). Do not give iron in the initial stabilization phase; add iron later during recovery once appetite improves.
Begin cautious feeding with WHO F-75 therapeutic milk (low-calorie, low-protein starter formula) in small, frequent feeds. After 2–7 days (when appetite returns and edema improves), transition to F-100 or ready-to-use therapeutic food (RUTF) for catch-up growth. Monitor closely for refeeding syndrome or fluid overload during this transition.
Lethargy, unconsciousness, or body temp < 35.5 °C in a malnourished child → possible hypoglycemia or sepsis; requires immediate glucose, warming, and urgent care.
No appetite despite severe malnutrition → indicates complicated SAM (often with infection); child needs inpatient care.
Worsening edema or difficulty breathing during feeding → suspect refeeding syndrome or incipient heart failure (slow down feeds, correct electrolytes).
Child with signs of malnutrition (wasting or edema) → measure weight/height and MUAC.
If WFH < –3 SD, MUAC < 11.5 cm, or bilateral pitting edema present → diagnose severe acute malnutrition (SAM).
Check for complications: assess for hypoglycemia, hypothermia, infection, dehydration, anemia, etc., and do an appetite test.
Classify: complicated SAM (edema, complications or poor appetite) → treat inpatient (WHO 10-step protocol). Uncomplicated SAM (no edema, appetite okay) → treat outpatient with therapeutic feeds.
In inpatient management: follow WHO steps (e.g., treat hypoglycemia/hypothermia, cautious rehydration, antibiotics, gentle feeding with F-75, then F-100) and monitor closely. In outpatient: provide high-energy RUTF and follow-up weekly until recovery.
Toddler in famine with bilateral leg edema, distended belly, 'flaky paint' rash, and reddish hair → Kwashiorkor.
18‑month‑old post-measles with poor appetite, pitting foot edema, and MUAC 10 cm → edematous malnutrition (kwashiorkor).
Case 1
A 2‑year‑old girl in a famine region is evaluated for leg swelling and rash.
Case 2
An 18‑month‑old boy who recently had measles is brought in with loss of appetite and swelling.
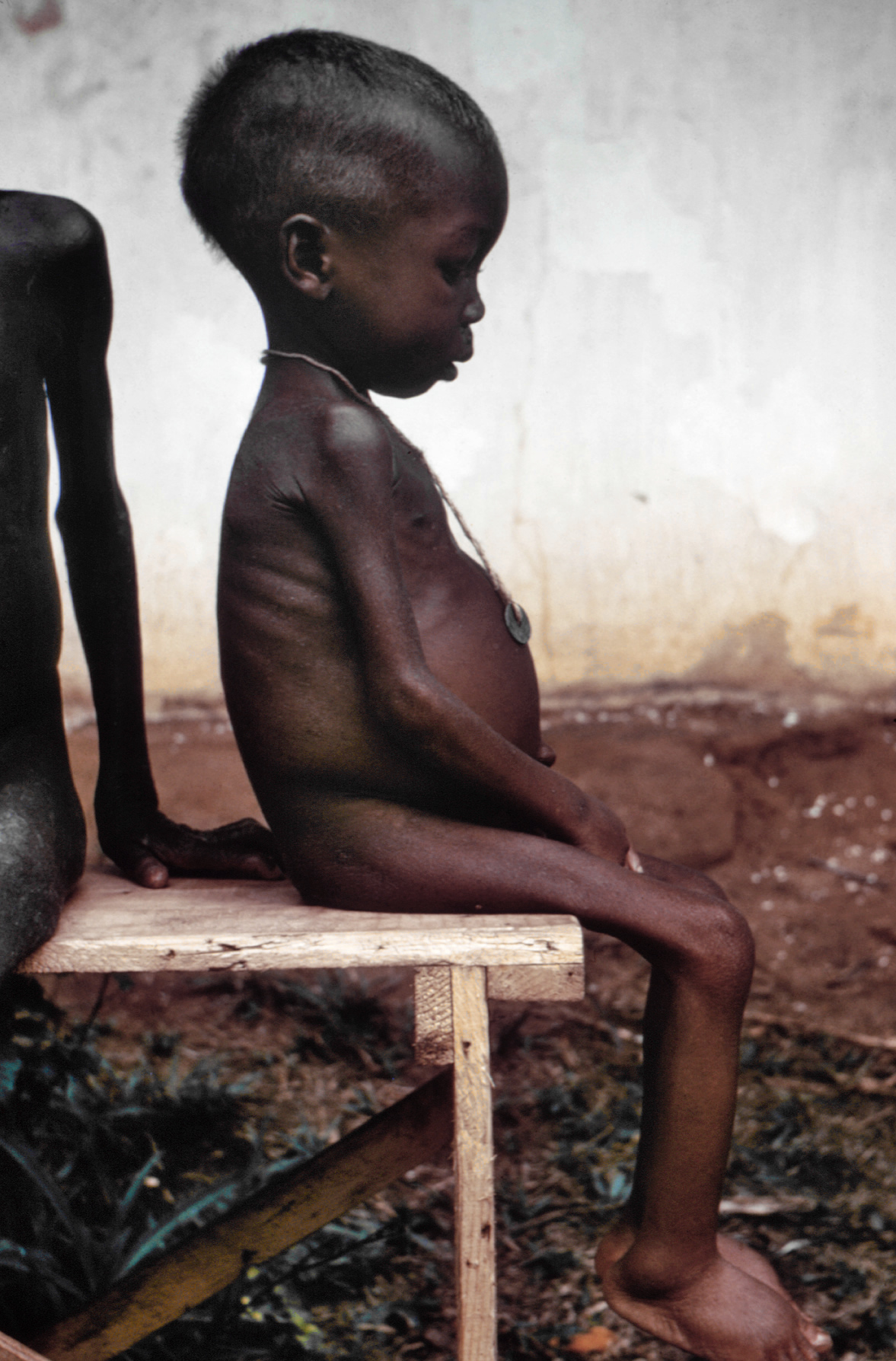
Child with Kwashiorkor: note edema in legs, distended abdomen, and muscle wasting masked by swelling.