Congenital discontinuity of the esophagus (ends in a blind pouch) that prevents swallowed material from reaching the stomach; often accompanied by a tracheoesophageal fistula (abnormal connection to the airway).
Life-threatening if not recognized early—newborns cannot feed and risk aspirating saliva/feeds. A classic neonatal surgical emergency and high-yield on boards.
Prenatal: polyhydramnios (excess amniotic fluid) due to fetal inability to swallow; ultrasound may show a small or absent stomach bubble.
At birth: excessive drooling and secretions; newborn immediately coughs, chokes, and turns cyanotic with first feeding (the classic "3 C's").
Nasogastric (NG) tube fails to pass into the stomach (meets obstruction ~10-12 cm from gums). X-ray reveals the NG tube coiled in a blind upper esophageal pouch.
If a distal TEF is present (most common type), the stomach and intestines fill with air (visible on X-ray); if no fistula, the abdomen remains gasless (scaphoid).
Often associated with other anomalies (consider VACTERL: Vertebral, imperforate Anus, Cardiac, Tracheo-Esophageal, Renal, Limb anomalies).
Do not feed a baby with suspected EA. Attempt to pass an NG tube; if it cannot reach the stomach, obtain an X-ray to confirm atresia (coiled tube in esophagus).
On X-ray, presence of abdominal gas helps identify the type: gas in stomach → distal TEF; no gas → pure EA (no fistula).
Stabilize the infant: keep NPO, position head upright (to minimize reflux), and use continuous suction to clear the esophageal pouch (prevent aspiration).
Evaluate for other anomalies given the high incidence of VACTERL association (e.g., echocardiogram, renal ultrasound, spinal radiographs).
Consult pediatric surgery for prompt repair. If the esophageal gap is too long for primary anastomosis, a staged approach (gastrostomy for feeding and later surgical repair) may be necessary.
Newborn turns cyanotic when feeding (can't breathe through nose) and pink when crying; difficulty passing a nasal catheter; NG tube passes to stomach normally.
Rare congenital cleft between larynx and esophagus → aspiration and recurrent pneumonia; feeding difficulty without esophageal obstruction.
Surgical repair is definitive: end-to-end esophageal anastomosis and closure of any fistula, typically within the first days of life.
Pre-op management: strict NPO, elevate head of bed, continuous suction of the upper pouch to prevent aspiration; provide IV fluids for hydration (and antibiotics if aspiration pneumonia is suspected).
If primary anastomosis is not possible (e.g., long-gap EA), a staged approach (e.g., gastrostomy feeding and later esophageal lengthening procedures) is used in specialized centers.
Post-repair, monitor for complications: esophageal strictures (may require dilation), recurrent TEF, or chronic gastroesophageal reflux (common in repaired EA).
3 C's of TEF: Coughing, Choking, Cyanosis with feeds.
Any newborn with cyanosis or respiratory distress during feeding → stop feeds immediately and evaluate for EA/TEF (to prevent aspiration and suffocation).
After surgical repair, persistent drooling or difficulty swallowing suggests an anastomotic stricture, and recurrent choking/coughing with feeds may indicate a recurrent fistula—both warrant prompt evaluation.
Newborn with drooling and choking on first feed → suspect EA/TEF.
Attempt NG tube placement: if tube cannot reach stomach, get X-ray to confirm a coiled tube in the esophagus.
If abdomen is gasless on X-ray → isolated esophageal atresia; if stomach gas is present → distal TEF likely.
Prevent aspiration (NPO, suction, upright position) and arrange surgical repair; concurrently screen for other VACTERL anomalies.
Full-term newborn (history of polyhydramnios) with drooling and choking/cyanosis on first feeding, and an NG tube that cannot be advanced into the stomach → esophageal atresia (likely with TEF).
Chest X-ray showing a coiled NG tube in the upper esophagus and air in the stomach → esophageal atresia with distal tracheoesophageal fistula (Gross type C, most common).
If X-ray shows a coiled NG tube but no gas in the abdomen → pure esophageal atresia without a fistula.
Case 1
A 1‑day‑old boy born at 39 weeks (mother had polyhydramnios) has excessive drooling and coughs with his first feeding, becoming cyanotic. An orogastric tube meets resistance 10 cm from the gums.
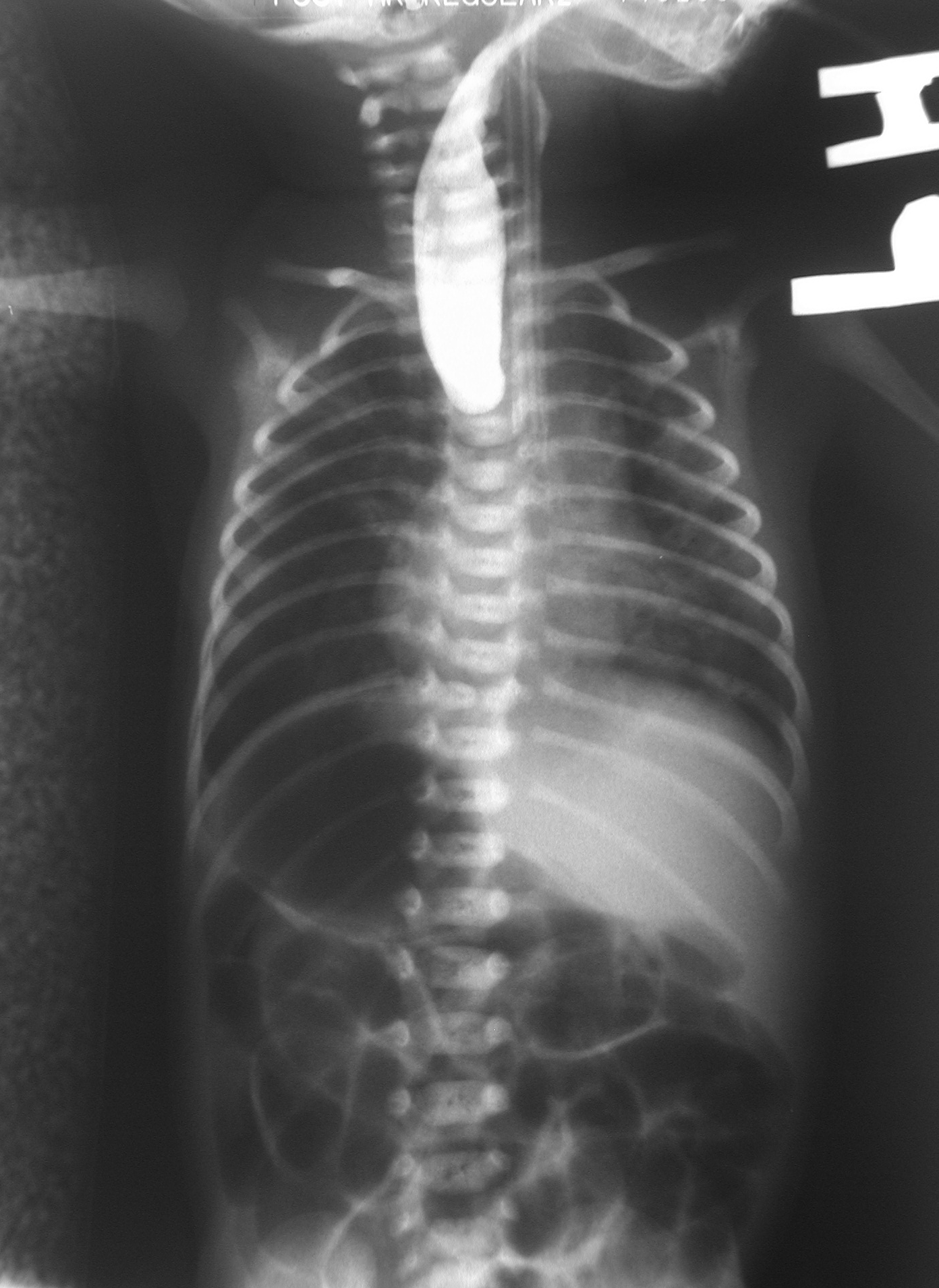
X-ray with contrast showing esophageal atresia: contrast fills the blind-ending upper esophageal pouch; none reaches the stomach.