Presence of blood in the urine (typically ≥3 RBCs/HPF on microscopy). Gross hematuria is visible blood (urine appearing red, pink, or tea-colored); microscopic hematuria is only detectable on urinalysis.
In adults, even mild hematuria can be the first sign of a serious problem (e.g., malignancy), so it should never be ignored. It's a common exam topic because its differential is broad (infections, stones, cancers, glomerular diseases) and it demands a systematic workup.
Often discovered as either gross hematuria (patient notices red, pink, or cola-colored urine) or microscopic hematuria (incidentally found on dipstick/microscopy).
Painful hematuria points to causes like stones or infection (e.g., flank pain with nephrolithiasis, dysuria with UTI), whereas painless hematuria is a red flag for malignancy (e.g., bladder cancer).
Glomerular hematuria (from kidney filters) tends to cause brown/tea-colored urine with dysmorphic RBCs, RBC casts, and possibly proteinuria; in contrast, bleeding from the ureters, bladder, or urethra is usually bright red and may include blood clots (no casts).
Verify true hematuria: repeat urinalysis with microscopy to confirm ≥3 RBC/HPF, and exclude false positives (menstrual blood, beet/pigment ingestion, muscle injury causing myoglobinuria).
Differentiate glomerular vs. non-glomerular source: glomerular origin is indicated by RBC casts, dysmorphic RBCs, and concurrent proteinuria (think nephritic syndrome), whereas normal-appearing RBCs or visible clots suggest an extraglomerular (urologic) source.
Use clinical clues: e.g., colicky flank pain → suspect a kidneystone; dysuria, fever → UTI; recent pharyngitis → consider post-streptococcal glomerulonephritis. Note that hematuria in an anticoagulated patient still warrants workup (anticoagulation can unmask an underlying lesion rather than being the sole cause).
Localize by timing of bleeding: initial hematuria (at start of urination) suggests a urethral source; terminal hematuria (at end of stream) points to bladder neck or prostate; total hematuria (throughout void) implies bleeding from the kidney or ureter.
Risk-stratify and investigate: All patients with gross hematuria or high-risk features (age >40, smoking history) require imaging of the urinary tract (often CT urography) and cystoscopy to evaluate for tumors or stones. Low-risk patients with isolated microscopic hematuria can be followed conservatively after an initial negative workup, but any new gross bleeding warrants re-evaluation.
Condition
Distinguishing Feature
Urinary tract infection
usually presents with dysuria, urgency, possibly fever; positive urine culture
Nephritic syndrome
glomerular hematuria with RBC casts, hypertension, edema, and proteinuria (e.g., post-streptococcal GN, IgA nephropathy)
Bladder cancer
classically painless gross hematuria in an older adult (especially smokers); often no other symptoms
Trauma
history of abdominal or flank injury (e.g., fall, motor vehicle accident) causing kidney or bladder damage
Address the underlying cause: e.g., antibiotics for UTI, lithotripsy or surgery for stones, stop offending drugs (like anticoagulants if safe), immunosuppressives for glomerulonephritis, or appropriate oncologic/surgical treatment for tumors (bladder or kidney cancer, BPH).
For significant gross hematuria with clot retention (patients unable to void due to clots), initiate bladder irrigation (place a large 3-way Foley catheter for continuous irrigation) and manually remove clots as needed to prevent obstruction.
If hematuria is asymptomatic and microscopic with no high-risk features, often no immediate intervention is needed apart from periodic monitoring (ensure it doesn't progress or indicate an evolving pathology).
Visible blood clots in urine point to a non-glomerular source (glomerular hematuria usually doesn't clot).
Don't dismiss hematuria in an older patient (even if on blood thinners) – painless hematuria is cancer until proven otherwise.
Painless gross hematuria (especially in adults >40 or smokers) – highly concerning for urothelial carcinoma (bladder or upper tract cancer) until proven otherwise; mandates prompt urologic evaluation.
Hematuria with unexplained weight loss or a flank mass – raises suspicion for renal cell carcinoma (kidney cancer).
Heavy hematuria with clots causing difficulty urinating – risk of bladder tamponade (urinary retention); this is a urologic emergency requiring urgent clot evacuation.
Dipstick positive for blood → confirm with microscopic exam (≥3 RBC/HPF); rule out benign causes like menses or exercise.
If infection is present (e.g., UTI), treat it and then recheck urine in a few weeks to ensure hematuria resolves (infection and malignancy can coexist).
If glomerular findings (proteinuria, casts, impaired kidney function), pursue nephrology workup (serologies for glomerulonephritis, consider kidney biopsy).
If no glomerular signs or gross hematuria, proceed with imaging (e.g., CT urography or renal ultrasound) to inspect kidneys/ureters, and perform cystoscopy to directly visualize the bladder.
If initial evaluation is unrevealing, continue to monitor periodically (repeat urinalysis in ~6–12 months). Educate patients to report any new episodes of gross hematuria immediately, as that would warrant repeat comprehensive evaluation.
Older male smoker with painless gross hematuria and no other symptoms → suspect bladder cancer (transitional cell carcinoma).
Sudden onset of unilateral flank pain radiating to the groin + hematuria → classic kidney stone (ureterolithiasis causing renal colic).
Cola-colored urine with RBC casts after a recent upper respiratory infection → indicates IgA nephropathy (Berger disease, a glomerular cause of hematuria).
Case 1
A 60‑year‑old man with a 40-pack-year smoking history reports intermittent episodes of red-colored urine. He has no pain, dysuria, or fevers. Physical exam is unremarkable.
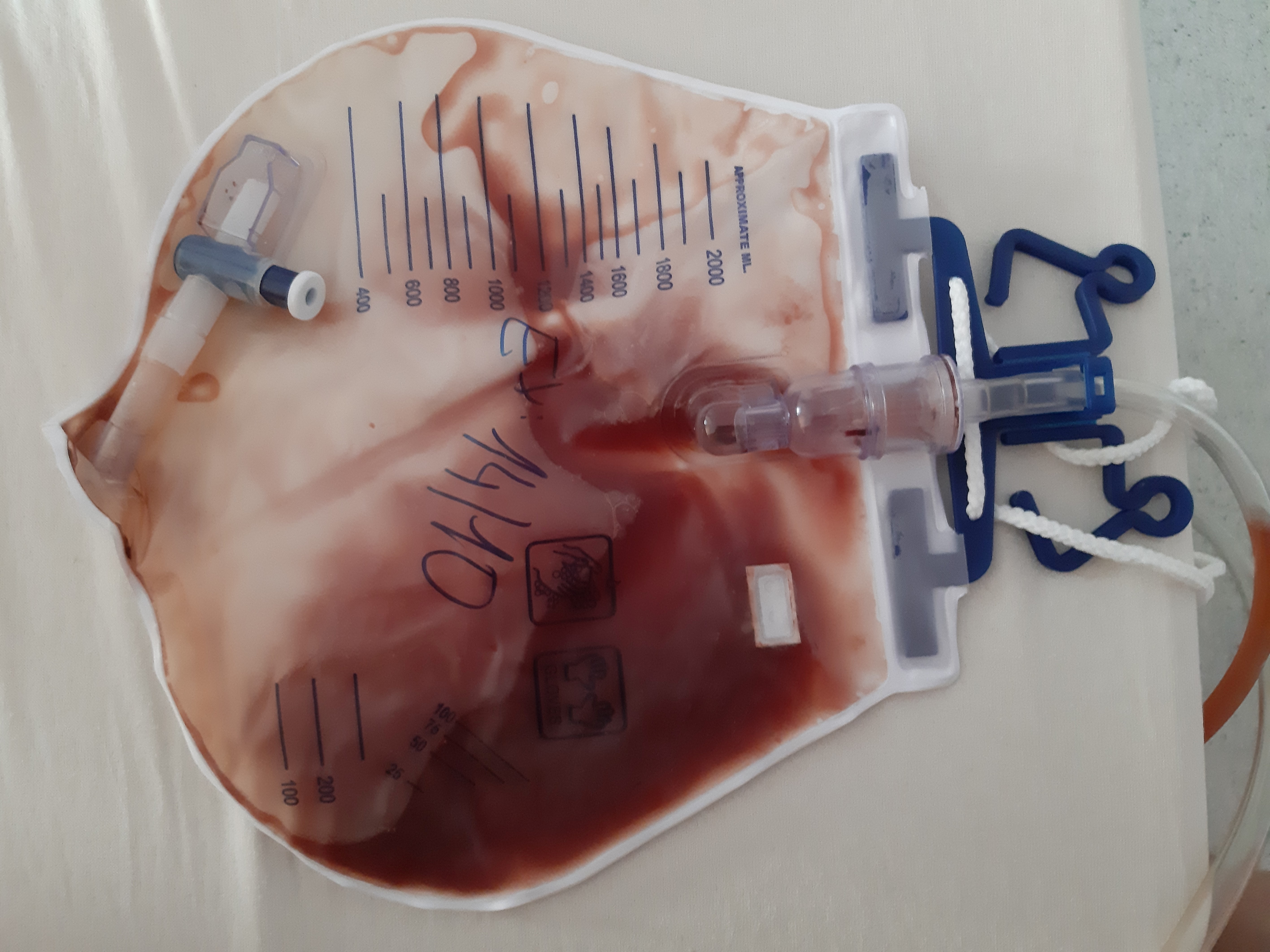
Gross hematuria (blood-tinged urine) collected in a urinary catheter bag.