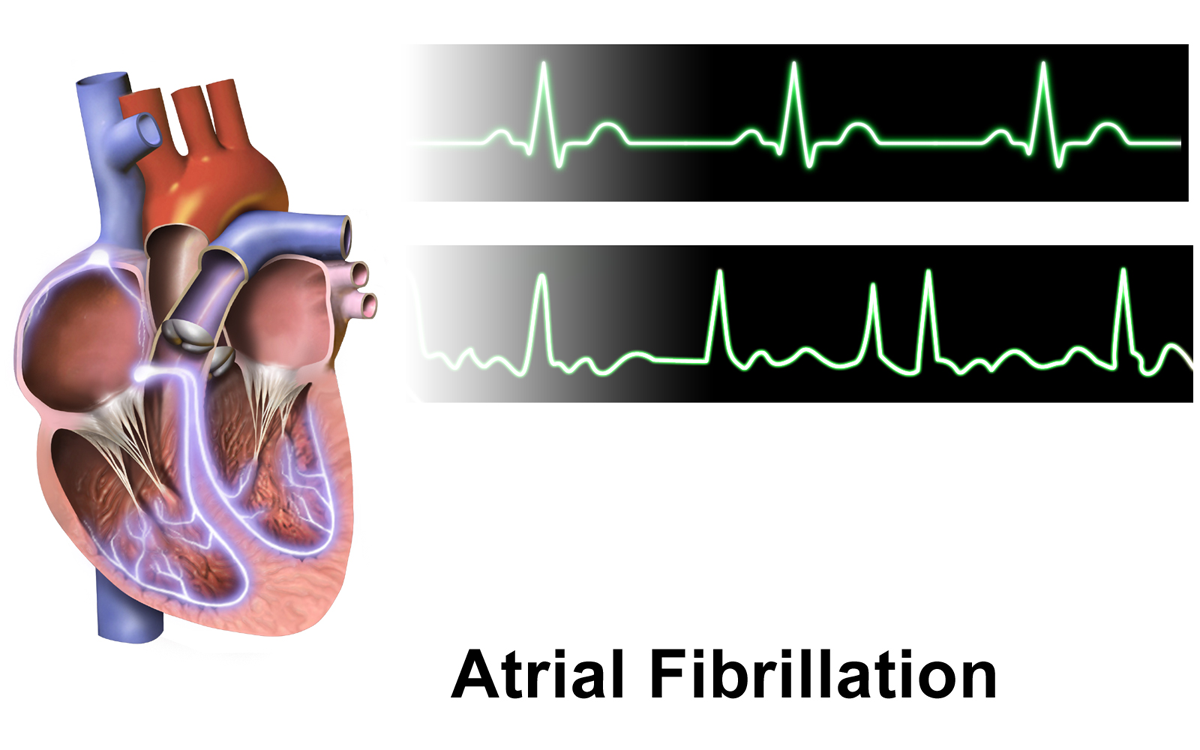
A supraventricular tachyarrhythmia caused by chaotic atrial electrical activity leading to ineffective atrial contraction and an irregularly irregular ventricular rhythm (no distinct P waves on ECG).
Most common sustained arrhythmia; associated with ≈5× higher stroke risk (atrial clots can embolize) and increased mortality. Can also cause heart failure (tachycardia-mediated cardiomyopathy) if uncontrolled. Frequent exam topic linking arrhythmia to stroke prevention.
Symptoms range from palpitations, anxiety, shortness of breath, or lightheadedness to syncope – or even asymptomatic (incidental). Pulse is classically irregularly irregular; apex heart rate may exceed peripheral pulse rate (pulse deficit).
Often in older patients with hypertension or structural heart disease (coronary artery disease, heart failure, valvular disease like rheumatic mitral stenosis). Other triggers: acute illness or infection, thyrotoxicosis (new AF + weight loss/tremor → check TSH), alcohol binge ('holiday heart'), surgery, pulmonary embolism.
Confirm diagnosis with ECG (absent P waves, irregularly spaced QRS complexes). Evaluate for precipitating causes: check TSH (hyperthyroidism), electrolytes, etc.
If stable: initiate rate control (e.g., IV beta blocker or diltiazem for rapid AF; digoxin if hypotensive or in systolic HF). Consider rhythm control (antiarrhythmics or elective cardioversion) for persistent symptoms, difficulty controlling rate, or in younger patients.
Estimate stroke risk with CHA₂DS₂-VASc score and decide on anticoagulation. Generally, ≥2 (men) or ≥3 (women) → chronic anticoagulation indicated (barring contraindications).
Perform a transthoracic echocardiogram to identify structural heart disease (e.g., valve stenosis, left atrial enlargement) and help guide management. If AF duration >48 h before planned cardioversion, patient needs 3 weeks of anticoagulation or a transesophageal echo to exclude atrial clot.
sawtooth atrial flutter waves (~300 bpm) often with regular 2:1 conduction (ventricular rate ~150)
Multifocal atrial tachycardia
irregular atrial rhythm but with ≥3 distinct P-wave morphologies on ECG (classically in COPD)
Rate control: β-blockers (e.g., metoprolol) or non-dihydropyridine calcium channel blockers (diltiazem) to slow AV conduction (goal <110 bpm at rest). Add digoxin in refractory cases or if concomitant HFrEF.
Rhythm control: consider cardioversion (electrical or pharmacologic) for new-onset or symptomatic AF. Antiarrhythmics (e.g., flecainide, sotalol, amiodarone) or catheter ablation can be used to maintain sinus rhythm in recurrent AF, especially in younger patients.
Anticoagulation: indicated for stroke prevention in eligible patients (per CHA₂DS₂-VASc). DOACs (direct oral anticoagulants like apixaban) are first-line for non-valvular AF. Use warfarin in valvular AF (e.g., mechanical valve or rheumatic MS).
Clue: Hyperthyroidism often presents as new-onset AF – always check a TSH level.
Mnemonic: CHA₂DS₂-VASc for stroke risk factors in AF: CHF, Hypertension, Age ≥75 (2 points), Diabetes, Stroke/TIA (2), Vascular disease, Age 65–74, Sex Category (female).
Irregularly irregular pulse with no P waves = atrial fibrillation until proven otherwise.
AF with hemodynamic instability (hypotension, pulmonary edema, chest pain) → emergency synchronized cardioversion is required.
AF with WPW (Wolff-Parkinson-White): irregular wide-complex tachycardia → avoid AV nodal blockers (risk of VF); use procainamide or immediate cardioversion.
Irregularly irregular pulse → get ECG to confirm AF (no P waves).
Elderly patient with long-standing hypertension and diabetes, now with palpitations, an irregularly irregular heartbeat, and absent P waves on ECG → Atrial fibrillation (rate control and anticoagulate as indicated).
Middle-aged patient with weight loss, tremor, and tachycardia is found to have AF → AF secondary to thyrotoxicosis (check TSH; treat the hyperthyroidism and use beta blockers).
Otherwise healthy adult with an episode of AF after heavy alcohol intake (holiday celebration) → 'Holiday heart' syndrome (paroxysmal AF triggered by alcohol binge).
Case 1
A 68‑year‑old man with hypertension and diabetes is evaluated for fatigue and an irregular heartbeat.
Case 2
A 45‑year‑old woman with weight loss, fine tremor, and insomnia develops new-onset rapid irregular palpitations.
Case 3
A 30‑year‑old man has an episode of heart palpitations the morning after an alcohol binge at a party.
Illustration of atrial fibrillation with chaotic atrial activity (irregular electrical signals) and irregular, rapid ventricular response on ECG.