Twisting of a loop of intestine around its mesentery, creating a closed-loop obstruction with risk of cutting off blood supply (ischemia/necrosis).
Surgical emergency—bowel necrosis can occur rapidly if not relieved. A classic cause of neonatal bilious vomiting and a common culprit in adult large bowel obstruction, often tested with its hallmark imaging signs and urgent management.
Neonates/infants: sudden bilious vomiting, abdominal distension, possibly bloody stools in a first-month infant → think midgut volvulus from malrotation.
Children: intermittent or chronic abdominal pain and vomiting can signal malrotation with partial volvulus; an acute midgut volvulus can still occur beyond infancy (less common but possible).
Adults: two main patterns—sigmoid volvulus (typically elderly, bedridden, chronic constipation; progressive abdominal distension, pain, obstipation) and cecal volvulus (younger adults, sometimes postpartum or with mobile cecum; acute right-sided colonic obstruction). Gastric volvulus (rare, often in older patients with paraesophageal hernia) presents with severe epigastric pain, retching, and inability to vomit.
Imaging is key: abdominal X-ray often shows diagnostic features (e.g., coffee bean sign – massively dilated loop in sigmoid volvulus). In infants, an upper GI contrast study can show a corkscrew/twisted duodenum in malrotation (if the baby is stable enough).
If volvulus is suspected with signs of ischemia (peritonitis, acidosis) or the patient is unstable, do not delay surgical intervention for imaging – proceed to OR.
For sigmoid volvulus without peritonitis, attempt endoscopic detorsion promptly (flexible sigmoidoscopy with rectal tube can relieve the twist in ~80–90%). Always plan definitive surgery after (sigmoid resection or fixation) due to high recurrence if only decompressed.
Cecal volvulus usually requires surgical correction (often right hemicolectomy or cecopexy) as endoscopic reduction is less successful. Gastric volvulus is a surgical emergency; an NG tube may be attempted for decompression, but definitive surgical repair (e.g., gastropexy) is usually needed.
Massive colonic dilation without mechanical twist, usually in ill older patients (no transition point on imaging).
Mesenteric ischemia
Older patient with afib or vascular disease, pain out of proportion but no obvious obstruction on imaging (arterial occlusion rather than volvulus).
Midgut volvulus (infant): Immediate surgical detorsion via Ladd's procedure (untwist bowel, cut Ladd's bands, reposition intestines, appendectomy) – do ASAP to prevent necrosis.
Sigmoid volvulus: If no peritonitis, perform urgent endoscopic reduction (sigmoidoscopic derotation and rectal tube). Follow up with elective sigmoid resection to prevent recurrence (mortality rises sharply if strangulation occurs).
Cecal volvulus: Primarily managed with surgery (often a right colectomy with anastomosis or cecopexy if bowel is viable). Endoscopic attempt at decompression is usually unsuccessful in cecal volvulus.
Gastric volvulus: Surgical emergency – attempt gastric decompression with NG tube, but definitive treatment is surgical (e.g., gastropexy or partial gastrectomy if necrotic).
Remember bilious emesis in an infant = malrotation with midgut volvulus until proven otherwise (surgical emergency).
Coffee bean sign: classic abdominal X-ray finding in sigmoid volvulus (dilated loop forms an inverted U shape with a central line).
Whirlpool sign: twisting of mesenteric vessels on CT (seen in midgut or cecal volvulus). Bird's beak sign: tapering of contrast or gas at the twist site (e.g., on barium enema or CT).
For gastric volvulus, think Borchardt's triad: unproductive retching, epigastric distension, and inability to pass an NG tube.
Bilious vomiting in any infant – presume malrotation/volvulus until ruled out (requires immediate evaluation).
Signs of possible bowel strangulation (fever, severe tenderness/peritonitis, hematochezia, acidosis, shock) → emergent surgery; do NOT delay for imaging or endoscopic attempts.
Suspect volvulus in acute obstruction: (a) Infant with bilious emesis or (b) Adult with acute abdominal distension/obstruction – obtain prompt imaging if stable.
If infant is stable: Upper GI series to confirm malrotation ("corkscrew" duodenum); if unstable or high suspicion, straight to OR for detorsion.
If sigmoid volvulus is seen on X-ray: no peritonitis → attempt endoscopic detorsion immediately; if successful, plan definitive surgical fix during same admission.
Any evidence of ischemia or unsuccessful endoscopic reduction (or diagnosis of cecal volvulus) → proceed to emergency surgery (resection or fixation as needed). Ensure aggressive fluid resuscitation and broad antibiotics if ischemic bowel is suspected.
A 3-week-old infant with sudden bilious projectile vomiting, abdominal distension, and blood in stool ± shock → Midgut volvulus due to malrotation (surgical emergency with Ladd's procedure).
A 70‑year‑old nursing home patient with a distended, tympanitic abdomen and obstipation. Abdominal X-ray shows an inverted U-shaped, distended colon loop (coffee bean sign) → Sigmoid volvulus (endoscopic decompression followed by surgical resection).
An elderly patient with paraesophageal hernia and acute epigastric pain, violent retching but no vomit, and inability to pass an NG tube → Gastric volvulus (Borchardt's triad; requires urgent surgery).
Case 1
A 1-month-old male infant presents with sudden onset of vomiting that turned bilious. He is irritable, with a distended abdomen and blood-streaked stools.
Case 2
A 75-year-old nursing home resident with a history of chronic constipation presents with 2 days of progressive abdominal bloating and crampy pain, now with nausea and no bowel movements or flatus.
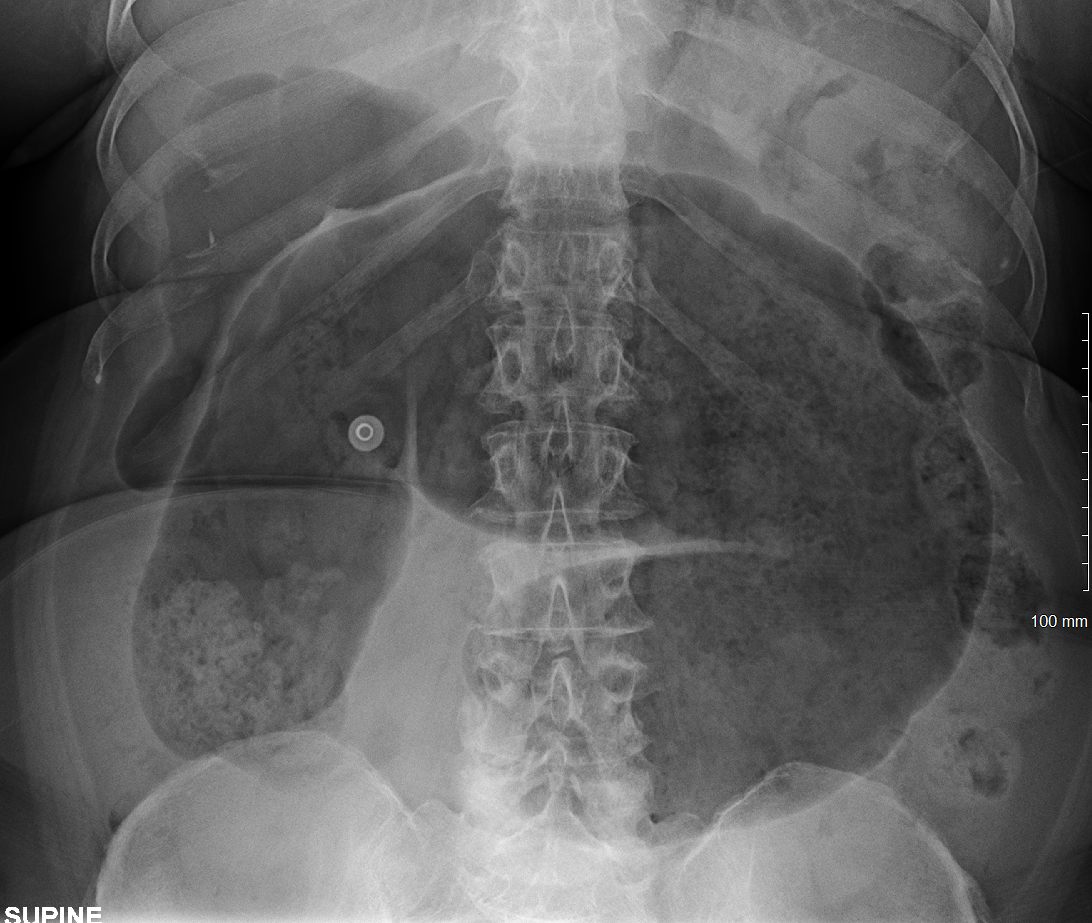
Supine abdominal X-ray showing a markedly distended air-filled cecum in cecal volvulus ("coffee bean" appearance in the right upper abdomen).