Injury to the median nerve (often at the elbow or wrist) leading to characteristic deficits; patients develop sensory loss in the lateral hand (thumb, index, middle, radial half of ring finger) and motor impairment of forearm/hand muscles (e.g., thenar muscle paralysis, inability to flex the index/thumb – "hand of benediction").
The median nerve controls thumb opposition and forearm flexion, so its injury causes significant functional impairment of the hand. Median nerve entrapment is common (carpal tunnel syndrome affects ~3% of adults) and frequently appears in exams featuring classic signs (thenar atrophy, ape hand, benediction sign) to test knowledge of hand innervation.
Proximal median nerve lesion (at or above elbow): Often due to trauma (e.g., supracondylar humerus fracture). Presents with inability to flex the thumb and index finger at the IP joints (giving a "hand of benediction" on attempted fist), weak forearm pronation, and loss of sensation in the thumb-index-middle fingers.
Distal median nerve lesion (wrist level): Classically from carpal tunnel syndrome (transverse ligament compression) or a deep wrist laceration. Forearm flexors are intact, but there is thenar eminence wasting with loss of thumb opposition ("ape hand" deformity) and numbness in the median nerve distribution of the hand (palmar thumb, index, middle, lateral ring finger).
In carpal tunnel syndrome, patients often have hand paresthesias that wake them at night, relieved by shaking the hand (flick sign). Exam shows positive Tinel's (tingling with percussion over the wrist) and Phalen's (symptoms with wrist flexion) tests. Chronic compression can lead to thenar weakness (difficulty with buttons, weak grip) and visible atrophy.
Localize the lesion by motor exam: inability to flex the index distal phalanx or pronate the forearm suggests a high lesion (median nerve injured above the forearm), whereas isolated thenar muscle weakness with intact forearm function points to a distal lesion at the wrist.
Use provocative tests for median neuropathy: Tinel's sign (tap over carpal tunnel to elicit tingling) and Phalen's maneuver (maximal wrist flexion to provoke symptoms) are typically positive in carpal tunnel syndrome. If diagnosis is unclear or surgery is planned, confirm with nerve conduction studies/EMG to pinpoint the site and severity.
Recognize that sensory symptoms usually precede motor findings in median nerve compression: patients develop numbness/tingling early, while weakness of the thenar muscles (thumb abduction/opposition) and atrophy occur later, indicating advanced injury.
Check sensation over the thenar eminence: in carpal tunnel syndrome, this area is spared (palmar cutaneous branch leaves the median nerve before the tunnel). Numbness in the thenar skin implies a lesion proximal to the wrist (e.g., pronator teres syndrome or cervical radiculopathy).
Numbness of medial 1½ digits (ring + little finger) with intrinsic hand muscle weakness; causes an "ulnar claw" posture of 4th/5th fingers at rest.
Cervical radiculopathy (C6/C7)
Neck pain with radicular arm symptoms; e.g., C6 root compression causes thumb/index finger numbness (often with altered reflexes) and a positive Spurling test.
Pronator teres syndrome
Proximal median nerve compression at elbow; causes forearm pain and includes sensory loss over the thenar eminence (unlike carpal tunnel).
Conservative management for compressive neuropathy: for carpal tunnel syndrome, start with wrist splinting (especially at night), activity modification, and possibly a local steroid injection. Treat contributing conditions (e.g., hypothyroidism, rheumatoid arthritis).
Surgical intervention if significant or refractory: for carpal tunnel, perform surgical release of the transverse carpal ligament if symptoms are severe (thenar weakness/atrophy or >6 months without improvement). For acute trauma (nerve laceration or entrapment in a fracture), prompt surgical repair or decompression of the median nerve is indicated. Postoperatively or in mild cases, physical therapy (nerve gliding exercises) aids functional recovery.
Hand of benediction vs ulnar claw: Benediction appears when making a fist (median nerve lesion – inability to flex first two digits), whereas an ulnar claw is seen at rest (ulnar nerve lesion – 4th/5th digit clawing).
LOAF muscles: The median nerve innervates the lateral hand intrinsics (Lumbricals 1–2, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis); loss of these in median palsy explains thenar eminence flattening and inability to flex the index IP joint.
Carpal tunnel spares thenar sensation: the palmar cutaneous branch of the median nerve branches off before the carpal tunnel, so sensation over the thenar eminence remains normal in CTS.
Progressive thenar atrophy or weakness (loss of thumb opposition) – indicates ongoing median nerve compression with axonal loss, warranting urgent evaluation (consider surgical decompression).
Acute median nerve injury with trauma (deep cut or fracture) – requires prompt surgical attention (to repair the nerve and prevent permanent deficits or neuroma formation).
Patient with hand numbness in median nerve distribution or relevant trauma → suspect median nerve injury.
Perform focused exam: test median nerve motor function (thumb opposition, finger flexion) and sensation in thumb/index/middle; use Phalen's and Tinel's tests if carpal tunnel is suspected.
If high lesion suspected (after elbow injury or with loss of forearm muscle function), immobilize and obtain surgical evaluation (for fracture reduction, nerve repair).
If signs point to carpal tunnel (typical history with positive tests), begin conservative therapy (night splints, rest, maybe steroid injection); address any reversible causes (e.g., endocrine).
Reassess frequently – if no improvement or if motor deficits emerge, get electrodiagnostics and proceed to surgical decompression of the nerve.
Child with a supracondylar humerus fracture who cannot flex the index and middle fingers ("hand of benediction" on making a fist) → median nerve injury at the elbow.
Middle-aged person with nocturnal tingling in the thumb, index, and middle fingers and thenar muscle wasting → carpal tunnel syndrome (median nerve compression at the wrist).
Case 1
A 52‑year‑old woman reports tingling and numbness in her right hand for 6 months.
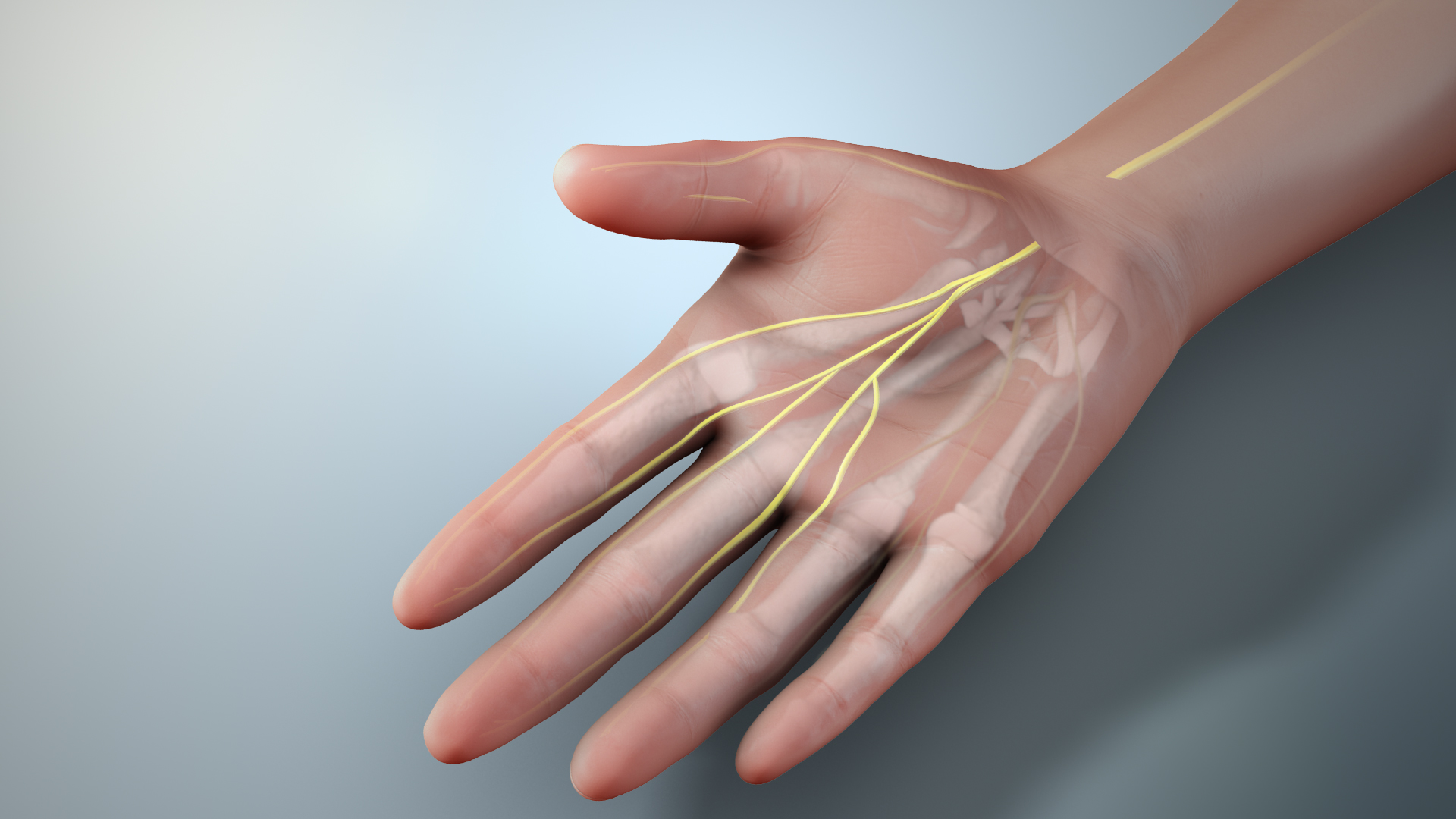
3D illustration showing the median nerve (yellow) passing through the carpal tunnel at the wrist into the hand.